On this page
- What the toilet anxiety statistics show
- Key Toilet Anxiety Statistics
- Who Was Included In The Toilet Anxiety Statistics?
- Behavioural Patterns
- Adult “Accident” History
- Symptom Duration
- Types Of Toilet Anxiety
- Previous Treatment
- Physical Diagnoses and IBS
- Treatment Sessions
- What These Statistics Suggest
- Related pages
What the toilet anxiety statistics show
This page summarises the key toilet anxiety statistics from the first 100 completed or closed anonymised clinical cases in the SICH Toilet Anxiety Research Project.
If you are looking for help rather than data, start with our main guide to hypnotherapy for toilet anxiety.
The data on this page is written as a plain English summary of the main numbers, not as the full research report.
For the full clinical findings, methodology, limitations and interpretation, read the SICH Toilet Anxiety Research Project.
It comes from clients who attended The Surrey Institute of Clinical Hypnotherapy where toilet anxiety was the primary presenting problem. The statistics show patterns we see again and again in people who seek specialist help, including long symptom duration, heavy use of safety behaviours, fear of not reaching a toilet in time, and loss of trust in the body.
This is not a population prevalence study. It does not tell us exactly how common toilet anxiety is in the general public. For that discussion, see our page on how common toilet anxiety is.
This page answers a different question:
What do the numbers show when people finally seek specialist help for toilet anxiety?

Key Toilet Anxiety Statistics
The data shows several clear patterns.
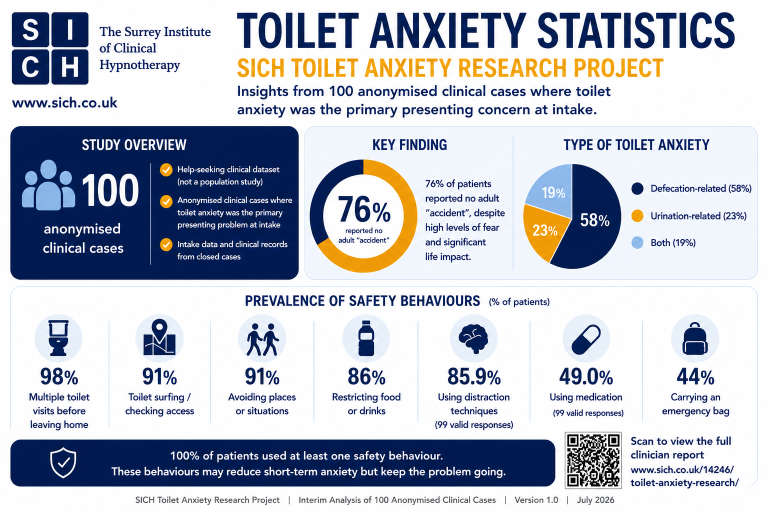
- The average reported symptom duration was 16 years.
- 76% reported no adult “accident”.
- 98% reported multiple toilet visits before leaving home.
- 91% reported toilet surfing or checking toilet access.
- 91% reported avoidance.
- 86% reported restricting food or drink.
- The average number of sessions was 4.96.
These are the headline numbers. They show a pattern of long duration, heavy safety behaviour use and fear organised around toilet access, urgency, uncertainty and loss of body trust.
Other figures, including age, sex split, presentation type and recorded physical diagnosis, are covered in the sections below.

Who Was Included In The Toilet Anxiety Statistics?
These statistics are part of the SICH Toilet Anxiety Research Project.
Each case involved a client who sought specialist help where toilet anxiety was the primary presenting problem.
The clients ranged in age from 16 to 83, with a mean age of 37. The sample was 58% female and 42% male.
That matters because toilet anxiety was not confined to one age group, one sex or one stage of life. It appeared in teenagers, working-age adults and older adults.
The shared pattern was not age, gender or lifestyle.
It was the fear of needing a toilet and not being able to get to one in time.
Behavioural Patterns
This is where the pattern becomes clearer. Many clients were not simply afraid of toilets. They were organising daily life around access, timing, escape and control. The pattern often included repeated toilet visits before leaving home, checking toilet locations, avoiding uncertain places, restricting food or drink, carrying emergency supplies, using distraction and, in some cases, using medication to feel safer before leaving the house.
On the surface, these behaviours can look practical. The person is trying to prevent panic, avoid embarrassment and stay in control.
But in toilet anxiety, the behaviour that feels protective can also become part of the trap.
Each time someone checks, avoids, restricts or prepares in order to feel safe, the brain can learn that the situation was only manageable because of the safety behaviour. The lesson becomes, “I got through that because I controlled everything.”
This is why behavioural patterns matter so much. The person may feel they are managing the problem, while the safety behaviours quietly teach the brain that ordinary situations are dangerous unless toilet access is known, immediate and controllable.
Medication As A Safety Behaviour
Medication use was recorded in almost half of valid cases, but this finding needs careful interpretation.
In many defecation-related cases, clients were using over-the-counter anti-diarrhoea medication such as Imodium as a way of trying to reduce the perceived risk of needing the toilet unexpectedly.
That means medication use in this dataset should not be read simply as evidence of medical treatment. In many cases, it appeared to sit within the wider pattern of safety behaviours, alongside checking toilet locations, restricting food or drink, going to the toilet repeatedly before leaving home, carrying emergency supplies and avoiding uncertain situations.
The important point is not the medication itself. It is what the medication was often being used for.
For many clients, it was another way to try to create certainty before leaving home.
Adult “Accident” History
This is the part many people do not expect. In the data, 76% of clients reported no adult “accident”. That matters because many people assume toilet anxiety must be caused by something terrible happening again and again. They imagine repeated accidents, repeated embarrassment, or repeated proof that the body cannot be trusted.
The data suggests a different pattern. For many clients, the fear was not driven by a long history of accidents. It was driven by the possibility of one happening.
That possibility can be enough to change behaviour. A person may begin checking toilets, avoiding journeys, leaving early, sitting near exits or restricting food and drink, not because something has happened many times before, but because the body has started reacting as though it could happen at any moment.
This is why toilet anxiety can feel so confusing. The person may know logically that they have usually managed to cope, but their body still reacts as though danger is close.
The toilet anxiety statistics do not suggest that accidents never matter. For some clients, a previous incident was part of the story. But the larger pattern is clear: toilet anxiety does not need repeated adult accidents to become severe, restrictive and life-limiting.
Symptom Duration
The statistics show that this is rarely a problem people seek help for quickly. The average reported symptom duration was 16 years.
That is a long time to live around a fear that many people never properly name.
For some clients, toilet anxiety had been present since childhood or adolescence. For others, it developed later and slowly became part of everyday life. Over time, the person may adapt around it so thoroughly that the coping pattern starts to feel normal.

They may choose routes based on toilet access, avoid certain journeys, sit near exits, decline invitations, restrict food or drink, or only feel comfortable when they know exactly where the nearest toilet is. From the outside, life may still look functional. Inside, it can involve constant calculation.
This is why the 16 year average matters. It suggests that toilet anxiety is often hidden, managed and worked around for many years before someone seeks specialist help.
The problem is not simply that people are frightened. It is that they can lose years of freedom while trying to keep the fear under control.
Types Of Toilet Anxiety
Toilet anxiety does not look identical in every client. Some people are terrified of needing a bowel movement away from home. Some are frightened of needing to urinate. Some live with both fears at the same time.
In the toilet anxiety statistics:
- 58% of clients presented with defecation-related toilet anxiety
- 23% with urination-related toilet anxiety
- 19% with both.
Those differences matter, but they can also be misleading.

One person may avoid eating before a journey because they are frightened of needing a poo. Another may stop drinking because they are frightened of needing to wee. Someone else may check every toilet on a route, not because they expect to use them all, but because not knowing where they are feels unsafe.
The details change.
The underlying fear is often the same.
What if I need a toilet and cannot get to one in time?
That is why toilet anxiety is not really defined by whether the fear is bowel-related, bladder-related or both. It is defined by the loss of trust in the body when toilet access feels uncertain.
This is also why people often describe the problem in different ways. Some call it travel anxiety. Some call it IBS anxiety. Some call it panic. Some just say they do not like being too far from a toilet.
The toilet anxiety statistics help show the common pattern underneath those different descriptions.
Previous Treatment
This section is important because it shows that many people reach specialist help without having previously received treatment that properly addressed toilet anxiety.
Previous treatment was discussed with clients as part of the clinical process. Across the toilet anxiety statistics, around 60% had no recorded previous treatment for the problem.
That matters.
It suggests that many people had lived with toilet anxiety for years before seeking targeted help. They may have adapted around it, avoided certain situations, changed routines, or simply tried to keep going without treatment.

For some clients, the problem had been approached through other labels, such as IBS, panic attacks, travel anxiety, social anxiety or a sensitive stomach. For others, it had not been formally treated at all.
This is one reason toilet anxiety can remain so entrenched. If the fear is not recognised as a specific pattern, the person may keep trying to manage the symptoms without addressing the core issue: the fear of needing a toilet and not being able to get to one in time.
The toilet anxiety statistics suggest that many clients were not looking for another coping strategy by the time they reached SICH. They were looking for someone who understood the pattern itself.
Physical Diagnoses and IBS
One of the biggest traps in toilet anxiety is believing the body is the problem.
This finding changes the way toilet anxiety is often understood. When the fear is felt in the body, it is easy to assume the body must be the whole problem. The urge feels real. The stomach sensations feel real. The bladder sensations feel real. The panic feels real. And they are real. But that does not always mean the problem is mainly physical.
But the toilet anxiety statistics point in a different direction.

Only 9% of clients had IBS or physical diagnosis alongside their toilet anxiety presentation.
That is a small number.
It means the majority of clients in this sample were not simply dealing with a diagnosed bowel or bladder condition. They were dealing with a fear pattern that made normal body signals feel dangerous when toilet access was uncertain.
That is the key difference.
At home, the body may feel manageable. Away from home, the same sensations can suddenly feel urgent, risky and impossible to ignore. A car journey, a queue, a meeting, a restaurant, a train, or anywhere without easy toilet access can turn an ordinary body signal into an alarm.
This is why toilet anxiety is so often misunderstood. The problem is not always that the body cannot be trusted. Very often, the problem is that the brain has learned to mistrust the body in the wrong situations.
The 9% figure matters because it challenges the assumption that toilet anxiety is usually a physical problem. For many clients, the real issue was not a faulty body.
It was a false alarm system.
Treatment Sessions
This is where the data becomes more hopeful. Long-standing toilet anxiety did not always mean long-term treatment. Across the closed cases, the average number of sessions was 4.96. That figure should not be read as a guarantee, a target, or a rule for every client. Some people changed more quickly, some needed longer, and more complex cases naturally required more individual work.
But the figure does matter.
Many clients had lived with toilet anxiety for years before seeking specialist help. The average reported symptom duration was 16 years. However, the number of years someone had lived with toilet anxiety did not meaningfully predict the number of sessions attended. In this dataset, long-term sufferers did not necessarily require longer courses of treatment.
That is the important point. A problem can be long-standing without being permanent.
For many clients, the issue was not that they lacked coping skills. They often had too many coping strategies already. The real problem was a learned fear pattern around urgency, access, escape and body trust.
When that pattern is recognised and treated directly, change can sometimes happen much faster than people expect.
The hopeful message in the treatment data is that toilet anxiety may have shaped someone’s life for years, but it does not automatically mean they need years of treatment.
What These Statistics Suggest
For many clients, the fear had become organised around urgency, access, escape, uncertainty and trust in the body. People were not simply reacting to what had happened before. They were often reacting to what they feared could happen if they were too far from a toilet, trapped, delayed, embarrassed or unable to leave.
That is why toilet anxiety can become so restrictive. A person may still be going to work, seeing family, travelling short distances or keeping life looking normal from the outside, while privately calculating toilets, routes, food, drink, exits and escape options.
The data also shows something important about hope. Many clients had lived with the problem for years, but long duration did not necessarily mean longer treatment. In many cases, the issue was not that the person needed better coping strategies. It was that the underlying fear pattern needed to be recognised and treated directly.
If you are looking for help with this problem, start with our main guide to hypnotherapy for toilet anxiety.
These toilet anxiety statistics point to one clear message: This is rarely just a toilet problem.